|
| ||||
|
On a possible prognostic value of otoacoustic emissions: A reprint of this article can be downloaded from here
1. INTRODUCTION Otoacoustic emissions (OAE) are known to mirror the functional status of the outer hair cells (OHC) of the inner ear which are one of the most important functional structures in the peripheral auditory system. Monitoring of OAEs is therefore employed for the detection of subtle changes of inner ear performance e.g. in the course of noise exposition or accompanying the therapy with ototoxic agents. The interest in the objective detectability of beginning or subclinical alterations in hearing status motivated the present investigation, in which the transitory evoked otoacoustic emissions (TEOAE) and the distortion product otoacoustic emissions (DPOAE) were monitored over a long time period in patients suffering from sudden hearing loss. In these patients, a notable alteration of hearing threshold within observable time intervals can be expected. Monitoring the OAEs together with clinical audiograms not only allows the evaluation of correlation between subjective and objective measures of hearing capability but it additionally offers the possibility to compare the results of early OAEs with later audiograms or early audiograms with later OAEs. Thus, two hypotheses can be tested: whether the OAEs recorded at one instance exhibit a kind of “memory” reflecting the functional deficits of the inner ear immediately after the sudden hearing loss or whether they could be able to anticipate the recovery of such deficits.
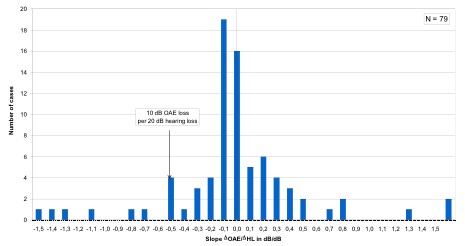
2. Materials and Methods Pure tone audiograms (PTA) and OAEs were examined in twenty-six ears of 25 patients suffering from sudden hearing loss from the first day to up to 505 days following the drop of hearing. The patients were selected out of 50 candidates according to the following criteria: one or both ears exhibit a systematic and significant recovery of pure tone threshold in at least one frequency, OAEs are detectable, a conductive hearing loss is excluded, and the auditory brainstem responses (ABR) yield no signs of retrocochlear disorders. TEOAEs and DPOAEs were measured under constant stimulus and recording conditions in three to nine sessions. The relation between OAE level and actual pure tone threshold was subject to a regression analysis. Only the responses fulfilling the above mentioned reproducibility or SNR criteria were included. The DPOAE level was plotted versus the hearing loss encountered at the frequency f2, whereas the TEOAE overall spectrum level was referred to the mean hearing threshold evaluated across 1 to 4 kHz. Besides the usual comparison of OAE and PTA explored on the same day, the OAE levels were also related to earlier and later subjective hearing loss (SHL). Furthermore, all points within the OAE/SHL-plane corresponding to one ear have been connected in chronological order to construct the individual “trajectory” of each ear. The slopes of these trajectories were analyzed statistically. Finally, the recovery of SHL as a function of the OAE level related to the initial hearing loss was considered. This analysis was motivated by the idea that large initial OAEs could be a predictor for a positive outcome and should hence be associated with a considerable threshold recovery. 3. RESULTS The correlation between OAE level and actual PTA is small but significant. Even smaller correlations are observed if the OAE level is related to former hearing loss, whereas the correlation improves if this parameter is compared to the SHL measured in a later session. The slopes of individual trajectories which connect the successive results of one ear in a plane defined by hearing loss and OAE level show a remarkable accumulation around zero, i.e. in many cases the OAEs remain unchanged even if the hearing loss decreases. This manifests itself as a pronounced peak around zero in the frequency distribution of the trajectory slopes (fig. 1).
Figure 1: Frequency distribution of the slopes DOAE / DHL (HL = hearing loss) of all trajectories describing the recovery of OAE and behavioral threshold after sudden hearing loss. The values cover the range from -1.8 to 8.3 dB / dB. The most important feature is the presence of a large peak at -0.1 dB / dB and a small local maximum at -0.5 dB / dB. The first one represents those ears, in which the threshold normalizes with only small or even absent alterations in OAE level, whereas the second one corresponds to the normal relation between OAE and threshold. 4. DISCUSSION The monitoring of TEOAE and DPOAE in patients with idiopathic sudden hearing loss during and after the treatment does not only give an insight into the recovery process of OHC function parallel with subjective hearing improvement but it also reveals paradoxical cases whose initial OAEs are unexpectedly large as compared to the corresponding hearing threshold. In many of these ears, the hearing threshold normalizes without a noticeable growth (or decrease) of OAE levels. The probability for a restitution of normal hearing is seen to be greater if the initial hearing loss related OAE level is large. Whether a reliable prognosis of outcome is possible on the basis of OAE testing remains to be proven in future investigations.
Figure 2: Recovery of behavioral hearing threshold as a function of the initial OAE level normalized to the hearing loss dependent reference level. The “normal” area and its upper limit (“reference level”) are explained in the text and shown schematically in the inset. Obviously, the probability for a recovery of hearing threshold tends to be larger if the OAE level lies in the upper range of the hearing loss related normal area or above it.
REFERENCES Brown AM, McDowell B, Forge A (1989) Acoustic distortion products can be used to monitor the effects of chronic gentamicin treatment. Hear Res 42: 143-156. About the Author
|